Diabetes complications
Diabetes complications can develop over time due to persistent high blood glucose levels and can cause damage to parts of your body including your eyes, heart, kidneys, or feet.
Diabetes complications can develop over time due to persistent high blood glucose levels and can cause damage to parts of your body including your eyes, heart, kidneys, or feet.

With regular screening, blood tests and effective diabetes management, the incidence of complications can be greatly reduced or prevented. Short term complications such us high blood glucose levels (hyperglycaemia) or low blood glucose levels (hypoglycaemia) are part of daily life with diabetes, and the risk of severe hypoglycemia and diabetes keto-acidosis (DKA), in particular in those with Type 1 diabetes, is always a side effect of insulin treatment (or the lack of it), and may occur rapidly.
Long-term complications such as retinopathy or neuropathy develop slowly and are a consequence of a long stretch of high glucose levels in your body. See below more information about diabetes long-term complications.
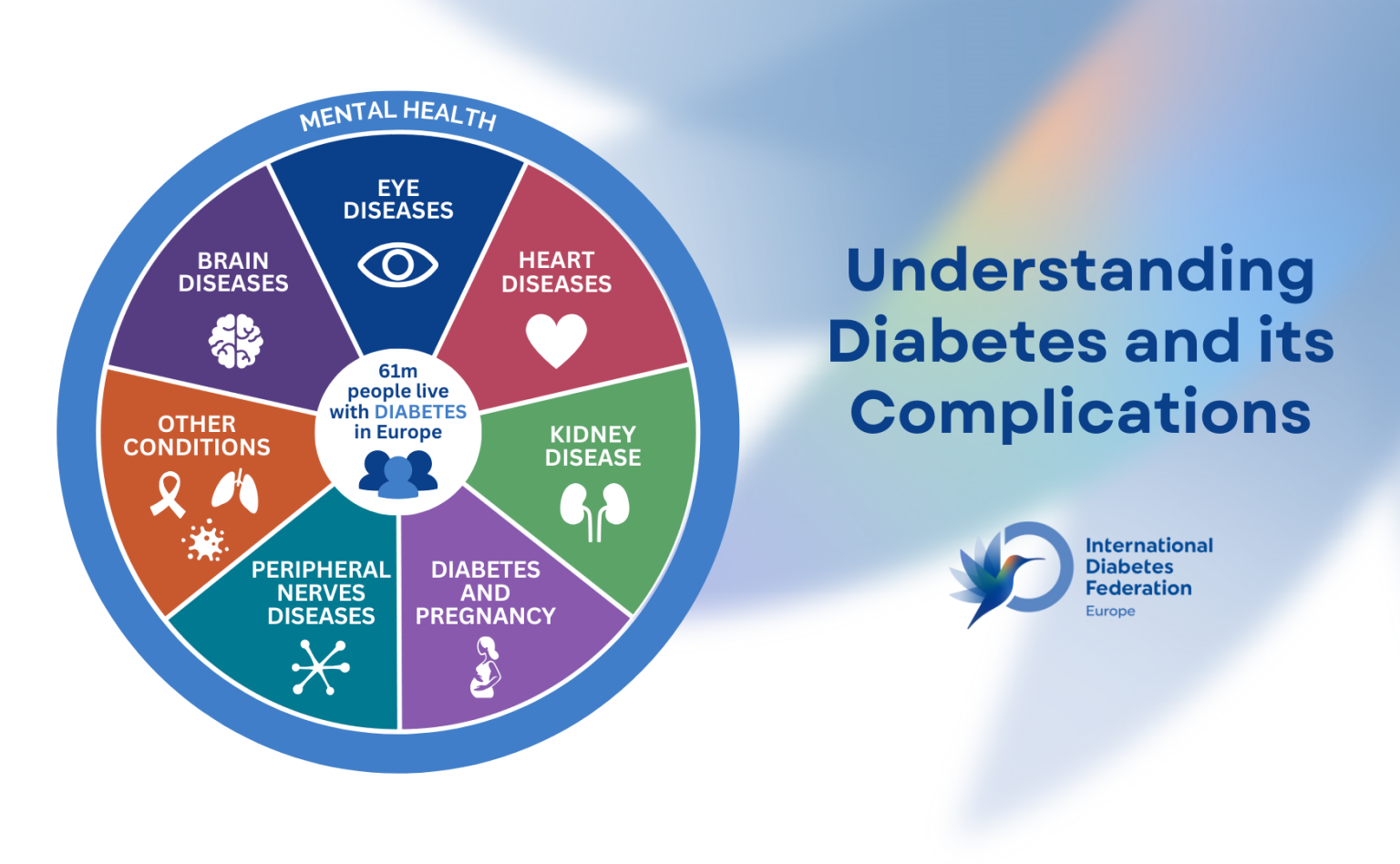
Diabetes long-term complications can be broken down into two categories;
International Diabetes Federation Europe prepared an illustration summarising the most common complications and comorbidities in people with diabetes.
Long-term complications can be prevented with accurate and effective diabetes management, good access to care, medicines and treatment the key is to keep glucose in recommended levels for the majority of time.
Diabetic Retinopathy is a serious eye complication of diabetes caused by damage to the small blood vessels of the retina, the light-sensitive tissue at the back of the eye.
If your blood glucose levels are consistently high, it can lead to this damage which can lead to vision loss and even blindness if not detected and treated early. When the blood vessels are damaged, they can swell and leak. High blood pressure and cholesterol can also increase your risk of eye problems.
To prevent complications in your eyes, you should:
Early stages often have no symptoms, which is why DiabeticRetina Screening is critical.
For more information visit www.diabeticretinascreen.ie, contact 1800 454555, or email info@diabeticretinascreen.ie.
Diabetic Nephropathy (also called diabetic kidney disease) is a progressive kidney condition caused by long-term high blood glucose levels. It is the leading cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) worldwide.
High blood sugar levels damage the tiny filtering units in the kidneys (called glomeruli), leading to:
Early Stage – Often silent (no symptoms), but urine tests may show:
A kidney health check is a quick and straightforward way to assess how well your kidneys are functioning. It can often be done at your GP or healthcare professional as part of a routine medical appointment.
Diabetic Neuropathy is a type of nerve damage caused by prolonged high blood sugar levels in people with diabetes. It affects up to 50% of people living with diabetes and can involve nerves in various parts of the body especially the legs and feet.
It can affect different types of nerves in your body, including in your feet, organs and muscles. Nerves carry messages between the brain and every part of our bodies so that we can see, hear, feel and move. They also carry signals to parts of the body such as the heart, making it beat at different speeds, and the lungs, so we can breathe.
Over time, high blood glucose levels can damage the small blood vessels that supply the nerves in your body. This stops essential nutrients reaching the nerves, which means the nerve fibres can become damaged, and they may disappear. This can cause problems in many different parts of your body, depending on the type of nerve affected.

Peripheral Neuropathy (most common)
See your GP or podiatrist at least once a year for a thorough foot exam. You may consider seeing our Diabetes Ireland podiatrist and get your feet checked in one of our clinics in Dublin and Cork. For more information click here.
Diabetes Ireland Care Centres, located in Dublin and Cork offer services including podiatry (footcare) and retinal eye screening for individuals living with diabetes.
Chronically high blood glucose levels can:
Risk Factors for CVD in People with Diabetes
This leads to a higher risk of:
Unfortunately, diabetes often occurs together with high blood pressure and high cholesterol. Therefore, when you have diabetes, it is essential that you monitor and manage both your blood pressure, cholesterol, and blood glucose levels.
Have your blood pressure checked at every doctor’s visit, at least:
For most people with diabetes, the target blood pressure is less than 140/90 mmHg. However, some individuals, especially those with kidney disease or had a previous cardiac event, may have a lower target, such as less than 130/80 mmHg, as recommended by their healthcare team.

Your GP or healthcare professional will measure your total cholesterol level as well as the different types of lipoproteins to assess whether you are at risk of artery disease.

The target level for diabetes is 48mmol/mol (6.5%).
Prediabetes level is 39mmol/mol-47mmol/mol. (6-6.5%)
Normal level is below 39mmol/mol. (<6%). Targets for older people may be individualised. Speak to your GP or healthcare professional about your HbA1c, know your numbers!
Peripheral Arterial Disease (PAD) and Peripheral Vascular Disease (PVD) are common and serious complications of diabetes. They involve narrowing or blockages of the arteries that supply blood to the legs and feet, usually due to atherosclerosis (plaque build up). Diabetes significantly increases the risk and severity of PAD/PVD.
How Diabetes Increases Risk of PVD/PAD
Symptoms of PAD/PVD in Diabetics
Symptoms may be silent in early stages, especially in people living with diabetes with neuropathy, but common signs include:
The treatment goals for peripheral artery disease (PAD) are:

Skin Conditions: Bacterial/fungal infections, diabetes dermopathy.
Diabetes-related dermopathy (often called “shin spots”) is a common skin condition that affects people who are living with diabetes.
Diabetes-related dermopathy looks like small, round pink, reddish or brown patches on your skin.
They can look like scars and be indented. They’re generally 1 centimetre to 2.5 centimetres in size.
The patches are harmless and don’t itch, ooze liquid, or cause pain. Diabetes-related dermopathy most often appears on the front of both your lower legs (on your shins), but one leg may have more patches than the other.
It can also appear on other parts of your body, such as your thighs and arms.
Gum disease also called periodontal gum disease, is the most common and serious mouth problem related to diabetes. Untreated, the disease advances in stages, from inflamed gums to tooth loss. High levels of blood glucose increase the risk that gum disease will progress from mild to severe.
See your dentist right away if you notice any signs or symptoms of mouth problems.
A healthy sexual relationship can be an important part of your life. While most people with diabetes can lead a normal sex life, diabetes may contribute to sexual problems for both men and women.
The most common problem for men is erectile dysfunction. This is where men have difficulty getting aroused long enough for intercourse due to reduced blood flow and nerve damage. There are many causes, such as being tired, stressed, depressed, or drinking too much alcohol. Erectile dysfunction can also be caused by certain medications taken for high blood pressure, depression, or stomach ulcers.
There are many ways to treat erectile dysfunction:
Chat with your doctor about all the options to decide what is best for you.
Much less is known about how diabetes affects women’s sexual health. What we do know are the main sexual problems that women, with or without diabetes, deal with:
It’s still unclear whether diabetes has any impact at all. But if you’re having a hard time coming to terms with living with diabetes, you’re more likely to experience sexual problems.
In most cases, keeping blood glucose levels within your target range will reduce your risk of thrush and urinary tract infection.
During periods or menopause, your blood glucose levels may change. We recommend speaking with your GP or diabetes educator to adjust your treatment.
Mental Health: People with diabetes have higher risk of developing mental health related problems such as depression, anxiety, or diabetes distress.
Read our special section about wellbeing and mental health and learn about our mental health and wellbeing support programmes.
